
Fetal Presentation, Position, and Lie (Including Breech Presentation)
- Variations in Fetal Position and Presentation |
During pregnancy, the fetus can be positioned in many different ways inside the mother's uterus. The fetus may be head up or down or facing the mother's back or front. At first, the fetus can move around easily or shift position as the mother moves. Toward the end of the pregnancy the fetus is larger, has less room to move, and stays in one position. How the fetus is positioned has an important effect on delivery and, for certain positions, a cesarean delivery is necessary. There are medical terms that describe precisely how the fetus is positioned, and identifying the fetal position helps doctors to anticipate potential difficulties during labor and delivery.
Presentation refers to the part of the fetus’s body that leads the way out through the birth canal (called the presenting part). Usually, the head leads the way, but sometimes the buttocks (breech presentation), shoulder, or face leads the way.
Position refers to whether the fetus is facing backward (occiput anterior) or forward (occiput posterior). The occiput is a bone at the back of the baby's head. Therefore, facing backward is called occiput anterior (facing the mother’s back and facing down when the mother lies on her back). Facing forward is called occiput posterior (facing toward the mother's pubic bone and facing up when the mother lies on her back).
Lie refers to the angle of the fetus in relation to the mother and the uterus. Up-and-down (with the baby's spine parallel to mother's spine, called longitudinal) is normal, but sometimes the lie is sideways (transverse) or at an angle (oblique).
For these aspects of fetal positioning, the combination that is the most common, safest, and easiest for the mother to deliver is the following:
Head first (called vertex or cephalic presentation)
Facing backward (occiput anterior position)
Spine parallel to mother's spine (longitudinal lie)
Neck bent forward with chin tucked
Arms folded across the chest
If the fetus is in a different position, lie, or presentation, labor may be more difficult, and a normal vaginal delivery may not be possible.
Variations in fetal presentation, position, or lie may occur when
The fetus is too large for the mother's pelvis (fetopelvic disproportion).
The uterus is abnormally shaped or contains growths such as fibroids .
The fetus has a birth defect .
There is more than one fetus (multiple gestation).

Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant person's spine) and with the face and body angled to one side and the neck flexed. Variations in fetal presentations include face, brow, breech, and shoulder. Occiput posterior position (facing forward, toward the mother's pubic bone) is less common than occiput anterior position (facing backward, toward the mother's spine). |
Variations in Fetal Position and Presentation
Some variations in position and presentation that make delivery difficult occur frequently.
Occiput posterior position
In occiput posterior position (sometimes called sunny-side up), the fetus is head first (vertex presentation) but is facing forward (toward the mother's pubic bone—that is, facing up when the mother lies on her back). This is a very common position that is not abnormal, but it makes delivery more difficult than when the fetus is in the occiput anterior position (facing toward the mother's spine—that is facing down when the mother lies on her back).
When a fetus faces up, the neck is often straightened rather than bent,which requires more room for the head to pass through the birth canal. Delivery assisted by a vacuum device or forceps or cesarean delivery may be necessary.
Breech presentation
In breech presentation, the baby's buttocks or sometimes the feet are positioned to deliver first (before the head).
When delivered vaginally, babies that present buttocks first are more at risk of injury or even death than those that present head first.
The reason for the risks to babies in breech presentation is that the baby's hips and buttocks are not as wide as the head. Therefore, when the hips and buttocks pass through the cervix first, the passageway may not be wide enough for the head to pass through. In addition, when the head follows the buttocks, the neck may be bent slightly backwards. The neck being bent backward increases the width required for delivery as compared to when the head is angled forward with the chin tucked, which is the position that is easiest for delivery. Thus, the baby’s body may be delivered and then the head may get caught and not be able to pass through the birth canal. When the baby’s head is caught, this puts pressure on the umbilical cord in the birth canal, so that very little oxygen can reach the baby. Brain damage due to lack of oxygen is more common among breech babies than among those presenting head first.
In a first delivery, these problems may occur more frequently because a woman’s tissues have not been stretched by previous deliveries. Because of risk of injury or even death to the baby, cesarean delivery is preferred when the fetus is in breech presentation, unless the doctor is very experienced with and skilled at delivering breech babies or there is not an adequate facility or equipment to safely perform a cesarean delivery.
Breech presentation is more likely to occur in the following circumstances:
Labor starts too soon (preterm labor).
The uterus is abnormally shaped or contains abnormal growths such as fibroids .
Other presentations
In face presentation, the baby's neck arches back so that the face presents first rather than the top of the head.
In brow presentation, the neck is moderately arched so that the brow presents first.
Usually, fetuses do not stay in a face or brow presentation. These presentations often change to a vertex (top of the head) presentation before or during labor. If they do not, a cesarean delivery is usually recommended.
In transverse lie, the fetus lies horizontally across the birth canal and presents shoulder first. A cesarean delivery is done, unless the fetus is the second in a set of twins. In such a case, the fetus may be turned to be delivered through the vagina.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

Appointments at Mayo Clinic
- Pregnancy week by week
- Fetal presentation before birth
The way a baby is positioned in the uterus just before birth can have a big effect on labor and delivery. This positioning is called fetal presentation.
Babies twist, stretch and tumble quite a bit during pregnancy. Before labor starts, however, they usually come to rest in a way that allows them to be delivered through the birth canal headfirst. This position is called cephalic presentation. But there are other ways a baby may settle just before labor begins.
Following are some of the possible ways a baby may be positioned at the end of pregnancy.
Head down, face down
When a baby is head down, face down, the medical term for it is the cephalic occiput anterior position. This the most common position for a baby to be born in. With the face down and turned slightly to the side, the smallest part of the baby's head leads the way through the birth canal. It is the easiest way for a baby to be born.

Head down, face up
When a baby is head down, face up, the medical term for it is the cephalic occiput posterior position. In this position, it might be harder for a baby's head to go under the pubic bone during delivery. That can make labor take longer.
Most babies who begin labor in this position eventually turn to be face down. If that doesn't happen, and the second stage of labor is taking a long time, a member of the health care team may reach through the vagina to help the baby turn. This is called manual rotation.
In some cases, a baby can be born in the head-down, face-up position. Use of forceps or a vacuum device to help with delivery is more common when a baby is in this position than in the head-down, face-down position. In some cases, a C-section delivery may be needed.

Frank breech
When a baby's feet or buttocks are in place to come out first during birth, it's called a breech presentation. This happens in about 3% to 4% of babies close to the time of birth. The baby shown below is in a frank breech presentation. That's when the knees aren't bent, and the feet are close to the baby's head. This is the most common type of breech presentation.
If you are more than 36 weeks into your pregnancy and your baby is in a frank breech presentation, your health care professional may try to move the baby into a head-down position. This is done using a procedure called external cephalic version. It involves one or two members of the health care team putting pressure on your belly with their hands to get the baby to roll into a head-down position.
If the procedure isn't successful, or if the baby moves back into a breech position, talk with a member of your health care team about the choices you have for delivery. Most babies in a frank breech position are born by planned C-section.

Complete and incomplete breech
A complete breech presentation, as shown below, is when the baby has both knees bent and both legs pulled close to the body. In an incomplete breech, one or both of the legs are not pulled close to the body, and one or both of the feet or knees are below the baby's buttocks. If a baby is in either of these positions, you might feel kicking in the lower part of your belly.
If you are more than 36 weeks into your pregnancy and your baby is in a complete or incomplete breech presentation, your health care professional may try to move the baby into a head-down position. This is done using a procedure called external cephalic version. It involves one or two members of the health care team putting pressure on your belly with their hands to get the baby to roll into a head-down position.
If the procedure isn't successful, or if the baby moves back into a breech position, talk with a member of your health care team about the choices you have for delivery. Many babies in a complete or incomplete breech position are born by planned C-section.

When a baby is sideways — lying horizontal across the uterus, rather than vertical — it's called a transverse lie. In this position, the baby's back might be:
- Down, with the back facing the birth canal.
- Sideways, with one shoulder pointing toward the birth canal.
- Up, with the hands and feet facing the birth canal.
Although many babies are sideways early in pregnancy, few stay this way when labor begins.
If your baby is in a transverse lie during week 37 of your pregnancy, your health care professional may try to move the baby into a head-down position. This is done using a procedure called external cephalic version. External cephalic version involves one or two members of your health care team putting pressure on your belly with their hands to get the baby to roll into a head-down position.
If the procedure isn't successful, or if the baby moves back into a transverse lie, talk with a member of your health care team about the choices you have for delivery. Many babies who are in a transverse lie are born by C-section.

If you're pregnant with twins and only the twin that's lower in the uterus is head down, as shown below, your health care provider may first deliver that baby vaginally.
Then, in some cases, your health care team may suggest delivering the second twin in the breech position. Or they may try to move the second twin into a head-down position. This is done using a procedure called external cephalic version. External cephalic version involves one or two members of the health care team putting pressure on your belly with their hands to get the baby to roll into a head-down position.
Your health care team may suggest delivery by C-section for the second twin if:
- An attempt to deliver the baby in the breech position is not successful.
- You do not want to try to have the baby delivered vaginally in the breech position.
- An attempt to move the baby into a head-down position is not successful.
- You do not want to try to move the baby to a head-down position.
In some cases, your health care team may advise that you have both twins delivered by C-section. That might happen if the lower twin is not head down, the second twin has low or high birth weight as compared to the first twin, or if preterm labor starts.

- Landon MB, et al., eds. Normal labor and delivery. In: Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021. https://www.clinicalkey.com. Accessed May 19, 2023.
- Holcroft Argani C, et al. Occiput posterior position. https://www.updtodate.com/contents/search. Accessed May 19, 2023.
- Frequently asked questions: If your baby is breech. American College of Obstetricians and Gynecologists https://www.acog.org/womens-health/faqs/if-your-baby-is-breech. Accessed May 22, 2023.
- Hofmeyr GJ. Overview of breech presentation. https://www.updtodate.com/contents/search. Accessed May 22, 2023.
- Strauss RA, et al. Transverse fetal lie. https://www.updtodate.com/contents/search. Accessed May 22, 2023.
- Chasen ST, et al. Twin pregnancy: Labor and delivery. https://www.updtodate.com/contents/search. Accessed May 22, 2023.
- Cohen R, et al. Is vaginal delivery of a breech second twin safe? A comparison between delivery of vertex and non-vertex second twins. The Journal of Maternal-Fetal & Neonatal Medicine. 2021; doi:10.1080/14767058.2021.2005569.
- Marnach ML (expert opinion). Mayo Clinic. May 31, 2023.
Products and Services
- A Book: Mayo Clinic Guide to a Healthy Pregnancy
- 3rd trimester pregnancy
- Fetal development: The 3rd trimester
- Overdue pregnancy
- Pregnancy due date calculator
- Prenatal care: Third trimester
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
- Healthy Lifestyle
5X Challenge
Thanks to generous benefactors, your gift today can have 5X the impact to advance AI innovation at Mayo Clinic.
Medical Information

Delivery, Face Presentation, and Brow Presentation: Understanding Fetal Positions and Birth Scenarios
Introduction:.
During childbirth, the position of the baby plays a significant role in the delivery process. While the most common fetal presentation is the head-down position (vertex presentation), variations can occur, such as face presentation and brow presentation. This comprehensive article aims to provide a thorough understanding of delivery, face presentation, and brow presentation, including their definitions, causes, complications, and management approaches.
Delivery Process:
- Normal Vertex Presentation: In a typical delivery, the baby is positioned head-down, with the back of the head (occiput) leading the way through the birth canal.
- Engagement and Descent: Prior to delivery, the baby's head engages in the pelvis and gradually descends, preparing for birth.
- Cardinal Movements: The baby undergoes a series of cardinal movements, including flexion, internal rotation, extension, external rotation, and restitution, which facilitate the passage through the birth canal.
Face Presentation:
- Definition: Face presentation occurs when the baby's face is positioned to lead the way through the birth canal instead of the vertex (head).
- Causes: Face presentation can occur due to factors such as abnormal fetal positioning, multiple pregnancies, uterine abnormalities, or maternal pelvic anatomy.
- Complications: Face presentation is associated with an increased risk of prolonged labor, difficulties in delivery, increased fetal malposition, birth injuries, and the need for instrumental delivery.
- Management: The management of face presentation depends on several factors, including the progression of labor, the size of the baby, and the expertise of the healthcare provider. Options may include closely monitoring the progress of labor, attempting a vaginal delivery with careful maneuvers, or considering a cesarean section if complications arise.
Brow Presentation:
- Definition: Brow presentation occurs when the baby's head is partially extended, causing the brow (forehead) to lead the way through the birth canal.
- Causes: Brow presentation may result from abnormal fetal positioning, poor engagement of the fetal head, or other factors that prevent full flexion or extension.
- Complications: Brow presentation is associated with a higher risk of prolonged labor, difficulty in descent, increased chances of fetal head entrapment, birth injuries, and the potential need for instrumental delivery or cesarean section.
- Management: The management of brow presentation depends on various factors, such as cervical dilation, progress of labor, fetal size, and the presence of complications. Close monitoring, expert assessment, and a multidisciplinary approach may be necessary to determine the safest delivery method, which can include vaginal delivery with careful maneuvers, instrumental assistance, or cesarean section if warranted.
Delivery Techniques and Intervention:
- Obstetric Maneuvers: In certain situations, skilled healthcare providers may use obstetric maneuvers, such as manual rotation or the use of forceps or vacuum extraction, to facilitate delivery, reposition the baby, or prevent complications.
- Cesarean Section: In cases where vaginal delivery is not possible or poses risks to the mother or baby, a cesarean section may be performed to ensure a safe delivery.
Conclusion:
Delivery, face presentation, and brow presentation are important aspects of childbirth that require careful management and consideration. Understanding the definitions, causes, complications, and appropriate management approaches associated with these fetal positions can help healthcare providers ensure safe and successful deliveries. Individualized care, close monitoring, and multidisciplinary collaboration are crucial in optimizing maternal and fetal outcomes during these unique delivery scenarios.
Hashtags: #Delivery #FacePresentation #BrowPresentation #Childbirth #ObstetricDelivery
On the Article

Krish Tangella MD, MBA

Alexander Enabnit

Alexandra Warren
Please log in to post a comment.
Related Articles
Test your knowledge, asked by users, related centers, related specialties, related physicians, related procedures, related resources, join dovehubs.
and connect with fellow professionals
Related Directories
At DoveMed, our utmost priority is your well-being. We are an online medical resource dedicated to providing you with accurate and up-to-date information on a wide range of medical topics. But we're more than just an information hub - we genuinely care about your health journey. That's why we offer a variety of products tailored for both healthcare consumers and professionals, because we believe in empowering everyone involved in the care process. Our mission is to create a user-friendly healthcare technology portal that helps you make better decisions about your overall health and well-being. We understand that navigating the complexities of healthcare can be overwhelming, so we strive to be a reliable and compassionate companion on your path to wellness. As an impartial and trusted online resource, we connect healthcare seekers, physicians, and hospitals in a marketplace that promotes a higher quality, easy-to-use healthcare experience. You can trust that our content is unbiased and impartial, as it is trusted by physicians, researchers, and university professors around the globe. Importantly, we are not influenced or owned by any pharmaceutical, medical, or media companies. At DoveMed, we are a group of passionate individuals who deeply care about improving health and wellness for people everywhere. Your well-being is at the heart of everything we do.
For Patients
For professionals, for partners.
Face and Brow Presentation
- Author: Teresa Marino, MD; Chief Editor: Carl V Smith, MD more...
- Sections Face and Brow Presentation
- Mechanism of Labor
- Labor Management
At the onset of labor, assessment of the fetal presentation with respect to the maternal birth canal is critical to the route of delivery. At term, the vast majority of fetuses present in the vertex presentation, where the fetal head is flexed so that the chin is in contact with the fetal thorax. The fetal spine typically lies along the longitudinal axis of the uterus. Nonvertex presentations (including breech, transverse lie, face, brow, and compound presentations) occur in less than 4% of fetuses at term. Malpresentation of the vertex presentation occurs if there is deflexion or extension of the fetal head leading to brow or face presentation, respectively.
In a face presentation, the fetal head and neck are hyperextended, causing the occiput to come in contact with the upper back of the fetus while lying in a longitudinal axis. The presenting portion of the fetus is the fetal face between the orbital ridges and the chin. The fetal chin (mentum) is the point designated for reference during an internal examination through the cervix. The occiput of a vertex is usually hard and has a smooth contour, while the face and brow tend to be more irregular and soft. Like the occiput, the mentum can present in any position relative to the maternal pelvis. For example, if the mentum presents in the left anterior quadrant of the maternal pelvis, it is designated as left mentum anterior (LMA).
In a brow presentation, the fetal head is midway between full flexion (vertex) and hyperextension (face) along a longitudinal axis. The presenting portion of the fetal head is between the orbital ridge and the anterior fontanel. The face and chin are not included. The frontal bones are the point of designation and can present (as with the occiput during a vertex delivery) in any position relative to the maternal pelvis. When the sagittal suture is transverse to the pelvic axis and the anterior fontanel is on the right maternal side, the fetus would be in the right frontotransverse position (RFT).
Face presentation occurs in 1 of every 600-800 live births, averaging about 0.2% of live births. Causative factors associated with a face presentation are similar to those leading to general malpresentation and those that prevent head flexion or favor extension. Possible etiology includes multiple gestations, grand multiparity, fetal malformations, prematurity, and cephalopelvic disproportion. At least one etiological factor may be identified in up to 90% of cases with face presentation.
Fetal anomalies such as hydrocephalus, anencephaly, and neck masses are common risk factors and may account for as many as 60% of cases of face presentation. For example, anencephaly is found in more than 30% of cases of face presentation. Fetal thyromegaly and neck masses also lead to extension of the fetal head.
A contracted pelvis or cephalopelvic disproportion, from either a small pelvis or a large fetus, occurs in 10-40% of cases. Multiparity or a large abdomen can cause decreased uterine tone, leading to natural extension of the fetal head.
Face presentation is diagnosed late in the first or second stage of labor by examination of a dilated cervix. On digital examination, the distinctive facial features of the nose, mouth, and chin, the malar bones, and particularly the orbital ridges can be palpated. This presentation can be confused with a breech presentation because the mouth may be confused with the anus and the malar bones or orbital ridges may be confused with the ischial tuberosities. The facial presentation has a triangular configuration of the mouth to the orbital ridges compared to the breech presentation of the anus and fetal genitalia. During Leopold maneuvers, diagnosis is very unlikely. Diagnosis can be confirmed by ultrasound evaluation, which reveals a hyperextended fetal neck. [ 1 , 2 ]
Brow presentation is the least common of all fetal presentations and the incidence varies from 1 in 500 deliveries to 1 in 1400 deliveries. Brow presentation may be encountered early in labor but is usually a transitional state and converts to a vertex presentation after the fetal neck flexes. Occasionally, further extension may occur resulting in a face presentation.
The causes of a persistent brow presentation are generally similar to those causing a face presentation and include cephalopelvic disproportion or pelvic contracture, increasing parity and prematurity. These are implicated in more than 60% of cases of persistent brow presentation. Premature rupture of membranes may precede brow presentation in as many as 27% of cases.
Diagnosis of a brow presentation can occasionally be made with abdominal palpation by Leopold maneuvers. A prominent occipital prominence is encountered along the fetal back, and the fetal chin is also palpable; however, the diagnosis of a brow presentation is usually confirmed by examination of a dilated cervix. The orbital ridge, eyes, nose, forehead, and anterior fontanelle are palpated. The mouth and chin are not palpable, thus excluding face presentation. Fetal ultrasound evaluation again notes a hyperextended neck.
As with face presentation, diagnosis is often made late in labor with half of cases occurring in the second stage of labor. The most common position is the mentum anterior, which occurs about twice as often as either transverse or posterior positions. A higher cesarean delivery rate occurs with a mentum transverse or posterior [ 3 ] position than with a mentum anterior position.
The mechanism of labor consists of the cardinal movements of engagement, descent, flexion, internal rotation, and the accessory movements of extension and external rotation. Intuitively, the cardinal movements of labor for a face presentation are not completely identical to those of a vertex presentation.
While descending into the pelvis, the natural contractile forces combined with the maternal pelvic architecture allow the fetal head to either flex or extend. In the vertex presentation, the vertex is flexed such that the chin rests on the fetal chest, allowing the suboccipitobregmatic diameter of approximately 9.5 cm to be the widest diameter through the maternal pelvis. This is the smallest of the diameters to negotiate the maternal pelvis. Following engagement in the face presentation, descent is made. The widest diameter of the fetal head negotiating the pelvis is the trachelobregmatic or submentobregmatic diameter, which is 10.2 cm (0.7 cm larger than the suboccipitobregmatic diameter). Because of this increased diameter, engagement does not occur until the face is at +2 station.
Fetuses with face presentation may initially begin labor in the brow position. Using x-ray pelvimetry in a series of 7 patients, Borrell and Ferstrom demonstrated that internal rotation occurs between the ischial spines and the ischial tuberosities, making the chin the presenting part, lower than in the vertex presentation. [ 4 , 5 ] Following internal rotation, the mentum is below the maternal symphysis, and delivery occurs by flexion of the fetal neck. As the face descends onto the perineum, the anterior fetal chin passes under the symphysis and flexion of the head occurs, making delivery possible with maternal expulsive forces.
The above mechanisms of labor in the term infant can occur only if the mentum is anterior and at term, only the mentum anterior face presentation is likely to deliver vaginally. If the mentum is posterior or transverse, the fetal neck is too short to span the length of the maternal sacrum and is already at the point of maximal extension. The head cannot deliver as it cannot extend any further through the symphysis and cesarean delivery is the safest route of delivery.
Fortunately, the mentum is anterior in over 60% of cases of face presentation, transverse in 10-12% of cases, and posterior only 20-25% of the time. Fetuses with the mentum transverse position usually rotate to the mentum anterior position, and 25-33% of fetuses with mentum posterior position rotate to a mentum anterior position. When the mentum is posterior, the neck, head and shoulders must enter the pelvis simultaneously, resulting in a diameter too large for the maternal pelvis to accommodate unless in the very preterm or small infant.
Three labor courses are possible when the fetal head engages in a brow presentation. The brow may convert to a vertex presentation, to a face presentation, or remain as a persistent brow presentation. More than 50% of brow presentations will convert to vertex or face presentation and labor courses are managed accordingly when spontaneous conversion occurs.
In the brow presentation, the occipitomental diameter, which is the largest diameter of the fetal head, is the presenting portion. Descent and internal rotation occur only with an adequate pelvis and if the face can fit under the pubic arch. While the head descends, it becomes wedged into the hollow of the sacrum. Downward pressure from uterine contractions and maternal expulsive forces may cause the mentum to extend anteriorly and low to present at the perineum as a mentum anterior face presentation.
If internal rotation does not occur, the occipitomental diameter, which measures 1.5 cm wider than the suboccipitobregmatic diameter and is thus the largest diameter of the fetal head, presents at the pelvic inlet. The head may engage but can descend only with significant molding. This molding and subsequent caput succedaneum over the forehead can become so extensive that identification of the brow by palpation is impossible late in labor. This may result in a missed diagnosis in a patient who presents later in active labor.
If the mentum is anterior and the forces of labor are directed toward the fetal occiput, flexing the head and pivoting the face under the pubic arch, there is conversion to a vertex occiput posterior position. If the occiput lies against the sacrum and the forces of labor are directed against the fetal mentum, the neck may extend further, leading to a face presentation.
The persistent brow presentation with subsequent delivery only occurs in cases of a large pelvis and/or a small infant. Women with gynecoid pelvis or multiparity may be given the option to labor; however, dysfunctional labor and cephalopelvic disproportion are more likely if this presentation persists.
Labor management of face and brow presentation requires close observation of labor progression because cephalopelvic disproportion, dysfunctional labor, and prolonged labor are much more common. As mentioned above, the trachelobregmatic or submentobregmatic diameters are larger than the suboccipitobregmatic diameter. Duration of labor with a face presentation is generally the same as duration of labor with a vertex presentation, although a prolonged labor may occur. As long as maternal or fetal compromise is not evident, labor with a face presentation may continue. [ 6 ] A persistent mentum posterior presentation is an indication for delivery by cesarean section.
Continuous electronic fetal heart rate monitoring is considered mandatory by many authors because of the increased incidence of abnormal fetal heart rate patterns and/or nonreassuring fetal heart rate patterns. [ 7 ] An internal fetal scalp electrode may be used, but very careful application of the electrode must be ensured. The mentum is the recommended site of application. Facial edema is common and can obscure the fetal facial anatomy and improper placement can lead to facial and ophthalmic injuries. Oxytocin can be used to augment labor using the same precautions as in a vertex presentation and the same criteria of assessment of uterine activity, adequacy of the pelvis, and reassuring fetal heart tracing.
Fetuses with face presentation can be delivered vaginally with overall success rates of 60-70%, while more than 20% of fetuses with face presentation require cesarean delivery. Cesarean delivery is performed for the usual obstetrical indications, including arrest of labor and nonreassuring fetal heart rate pattern.
Attempts to manually convert the face to vertex (Thom maneuver) or to rotate a posterior position to a more favorable anterior mentum position are rarely successful and are associated with high fetal morbidity and mortality and maternal morbidity, including cord prolapse, uterine rupture, and fetal cervical spine injury with neurological impairment. Given the availability and safety of cesarean delivery, internal rotation maneuvers are no longer justified unless cesarean section cannot be readily performed.
Internal podalic version and breech extraction are also no longer recommended in the modern management of the face presentation. [ 8 ]
Operative delivery with forceps must be approached with caution. Since engagement occurs when the face is at +2 position, forceps should only be applied to the face that has caused the perineum to bulge. Increased complications to both mother and fetus can occur [ 9 ] and operative delivery must be approached with caution or reserved when cesarean section is not readily available. Forceps may be used if the mentum is anterior. Although the landmarks are different, the application of any forceps is made as if the fetus were presenting directly in the occiput anterior position. The mouth substitutes for the posterior fontanelle, and the mentum substitutes for the occiput. Traction should be downward to maintain extension until the mentum passes under the symphysis, and then gradually elevated to allow the head to deliver by flexion. During delivery, hyperextension of the fetal head should be avoided.
As previously mentioned, the persistent brow presentation has a poor prognosis for vaginal delivery unless the fetus is small, premature, or the maternal pelvis is large. Expectant management is reasonable if labor is progressing well and the fetal well-being is assessed, as there can be spontaneous conversion to face or vertex presentation. The earlier in labor that brow presentation is diagnosed, the higher the likelihood of conversion. Minimal intervention during labor is recommended and some feel the use of oxytocin in the brow presentation is contraindicated.
The use of operative vaginal delivery or manual conversion of a brow to a more favorable presentation is contraindicated as the risks of perinatal morbidity and mortality are unacceptably high. Prolonged, dysfunctional, and arrest of labor are common, necessitating cesarean section delivery.
The incidence of perinatal morbidity and mortality and maternal morbidity has decreased due to the increased incidence of cesarean section delivery for malpresentation, including face and brow presentation.
Neonates delivered in the face presentation exhibit significant facial and skull edema, which usually resolves within 24-48 hours. Trauma during labor may cause tracheal and laryngeal edema immediately after delivery, which can result in neonatal respiratory distress. In addition, fetal anomalies or tumors, such as fetal goiters that may have contributed to fetal malpresentation, may make intubation difficult. Physicians with expertise in neonatal resuscitation should be present at delivery in the event that intubation is required. When a fetal anomaly has been previously diagnosed by ultrasonographic evaluation, the appropriate pediatric specialists should be consulted and informed at time of labor.
Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol . 2017 Dec. 217 (6):633-41. [QxMD MEDLINE Link] .
[Guideline] Ghi T, Eggebø T, Lees C, et al. ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound Obstet Gynecol . 2018 Jul. 52 (1):128-39. [QxMD MEDLINE Link] . [Full Text] .
Shaffer BL, Cheng YW, Vargas JE, Laros RK Jr, Caughey AB. Face presentation: predictors and delivery route. Am J Obstet Gynecol . 2006 May. 194(5):e10-2. [QxMD MEDLINE Link] .
Borell U, Fernstrom I. The mechanism of labour. Radiol Clin North Am . 1967 Apr. 5(1):73-85. [QxMD MEDLINE Link] .
Borell U, Fernstrom I. The mechanism of labour in face and brow presentation: a radiographic study. Acta Obstet Gynecol Scand . 1960. 39:626-44.
Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand . 2011 May. 90(5):540-2. [QxMD MEDLINE Link] .
Collaris RJ, Oei SG. External cephalic version: a safe procedure? A systematic review of version-related risks. Acta Obstet Gynecol Scand . 2004 Jun. 83(6):511-8. [QxMD MEDLINE Link] .
Verspyck E, Bisson V, Gromez A, Resch B, Diguet A, Marpeau L. Prophylactic attempt at manual rotation in brow presentation at full dilatation. Acta Obstet Gynecol Scand . 2012 Nov. 91(11):1342-5. [QxMD MEDLINE Link] .
Johnson JH, Figueroa R, Garry D. Immediate maternal and neonatal effects of forceps and vacuum-assisted deliveries. Obstet Gynecol . 2004 Mar. 103(3):513-8. [QxMD MEDLINE Link] .
Benedetti TJ, Lowensohn RI, Truscott AM. Face presentation at term. Obstet Gynecol . 1980 Feb. 55(2):199-202. [QxMD MEDLINE Link] .
BROWNE AD, CARNEY D. OBSTETRICS IN GENERAL PRACTICE. MANAGEMENT OF MALPRESENTATIONS IN OBSTETRICS. Br Med J . 1964 May 16. 1(5393):1295-8. [QxMD MEDLINE Link] .
Campbell JM. Face presentation. Aust N Z J Obstet Gynaecol . 1965 Nov. 5(4):231-4. [QxMD MEDLINE Link] .

Contributor Information and Disclosures
Teresa Marino, MD Assistant Professor, Attending Physician, Division of Maternal-Fetal Medicine, Tufts Medical Center Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Received salary from Medscape for employment. for: Medscape.
Carl V Smith, MD The Distinguished Chris J and Marie A Olson Chair of Obstetrics and Gynecology, Professor, Department of Obstetrics and Gynecology, Senior Associate Dean for Clinical Affairs, University of Nebraska Medical Center Carl V Smith, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , American Institute of Ultrasound in Medicine , Association of Professors of Gynecology and Obstetrics , Central Association of Obstetricians and Gynecologists , Society for Maternal-Fetal Medicine , Council of University Chairs of Obstetrics and Gynecology , Nebraska Medical Association Disclosure: Nothing to disclose.
Chitra M Iyer, MD, Perinatologist, Obstetrix Medical Group, Fort Worth, Texas.
Chitra M Iyer, MD is a member of the following medical societies: American College of Obstetricians and Gynecologists , Society of Maternal-Fetal Medicine .
Disclosure: Nothing to disclose.
What would you like to print?
- Print this section
- Print the entire contents of
- Print the entire contents of article
- HIV in Pregnancy
- Anemia and Thrombocytopenia in Pregnancy
- Pulmonary Disease and Pregnancy
- Adrenal Disease and Pregnancy
- Cardiovascular Disease and Pregnancy
- Kidney Disease and Pregnancy
- Pregnancy After Transplantation
- Is immunotherapy for cancer safe in pregnancy?
- Labetalol, Nifedipine: Outcome on Pregnancy Hypertension
- The Pregnancy Challenges of Women With Chronic Conditions

- Drug Interaction Checker
- Pill Identifier
- Calculators

- 2020/viewarticle/immunotherapy-cancer-safe-pregnancy-2024a100083dnews news Is immunotherapy for cancer safe in pregnancy?

- 2002261369-overviewDiseases & Conditions Diseases & Conditions Postterm Pregnancy


- Physician Physician Board Reviews Physician Associate Board Reviews CME Lifetime CME Free CME MATE and DEA Compliance
- Student USMLE Step 1 USMLE Step 2 USMLE Step 3 COMLEX Level 1 COMLEX Level 2 COMLEX Level 3 96 Medical School Exams Student Resource Center NCLEX - RN NCLEX - LPN/LVN/PN 24 Nursing Exams
- Nurse Practitioner APRN/NP Board Reviews CNS Certification Reviews CE - Nurse Practitioner FREE CE
- Nurse RN Certification Reviews CE - Nurse FREE CE
- Pharmacist Pharmacy Board Exam Prep CE - Pharmacist
- Allied Allied Health Exam Prep Dentist Exams CE - Social Worker CE - Dentist
- Point of Care
- Free CME/CE
Delivery, Face and Brow Presentation
Introduction.
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference. Face presentation is an abnormal form of cephalic presentation where the presenting part is the mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3] In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation, with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, and black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, and polyhydramnios. [2] [4] [5] These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. Palpating orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation is possible. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, the anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse. Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] Ultrasound imaging can show a reduced angle between the occiput and the spine or the chin is separated from the chest. However, ultrasound does not provide much predictive value for the outcome of labor. [7]
Anatomy and Physiology
Register for free and read the full article, learn more about a subscription to statpearls point-of-care.
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The 3 most important planes in the female pelvis are the pelvic inlet, mid-pelvis, and pelvic outlet. Four diameters can describe the pelvic inlet: anteroposterior, transverse, and 2 obliques. Furthermore, based on the landmarks on the pelvic inlet, there are 3 different anteroposterior diameters named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these 3 diameters is obstetrical conjugate, which measures approximately 10.5 cm and is the distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5 cm and is the widest distance between the innominate line on both sides. The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are 6 distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the diameter presented in the vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5 cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the diameter in the face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5 cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some key movements are impossible in the face or brow presentations. Based on the information provided above, it is obvious that labor be arrested in brow presentation unless it spontaneously changes to the face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery are explained in later sections.
Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore, the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations. Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous. Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] External transducer devices are advised to prevent damage to the eyes. When internal monitoring is inevitable, monitoring devices on bony parts should be placed carefully.
Consultations that are typically requested for patients with delivery of face/brow presentation include the following:
- Experienced midwife, preferably looking after laboring women 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (eg, epidural)
- Theatre team - in case of failure to progress, an emergency cesarean section is required.
Preparation
No specific preparation is required for face or brow presentation. However, discussing the labor options with the mother and birthing partner and informing members of the neonatal, anesthetic, and theatre co-ordinating teams is essential.
Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and the pressure of the amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery. If the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
The pubis is described as mentum-anterior when the fetal chin is rotated towards the maternal symphysis. In these cases, further descent through the vaginal canal continues, with approximately 73% of cases delivering spontaneously. [9] The fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot occur. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10] However, some complications are still associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor. Prolonged labor itself can provoke fetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications. Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5 cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head engages later, and labor progresses more slowly. Failure to progress in labor is also more common in both presentations compared to the vertex presentation. Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descending through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section. Manual attempts to change face presentation to vertex or manual or forceps rotation to mentum anterior are considered dangerous and discouraged.
Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta obstetricia et gynecologica Scandinavica. 2011 May:90(5):540-2. doi: 10.1111/j.1600-0412.2011.01105.x. Epub [PubMed PMID: 21501123]
Tapisiz OL, Aytan H, Altinbas SK, Arman F, Tuncay G, Besli M, Mollamahmutoglu L, Danışman N. Face presentation at term: a forgotten issue. The journal of obstetrics and gynaecology research. 2014 Jun:40(6):1573-7. doi: 10.1111/jog.12369. Epub [PubMed PMID: 24888918]
Zayed F, Amarin Z, Obeidat B, Obeidat N, Alchalabi H, Lataifeh I. Face and brow presentation in northern Jordan, over a decade of experience. Archives of gynecology and obstetrics. 2008 Nov:278(5):427-30. doi: 10.1007/s00404-008-0600-0. Epub 2008 Feb 19 [PubMed PMID: 18283473]
Bashiri A,Burstein E,Bar-David J,Levy A,Mazor M, Face and brow presentation: independent risk factors. The journal of maternal-fetal [PubMed PMID: 18570114]
Shaffer BL, Cheng YW, Vargas JE, Laros RK Jr, Caughey AB. Face presentation: predictors and delivery route. American journal of obstetrics and gynecology. 2006 May:194(5):e10-2 [PubMed PMID: 16647888]
Bellussi F, Ghi T, Youssef A, Salsi G, Giorgetta F, Parma D, Simonazzi G, Pilu G. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. American journal of obstetrics and gynecology. 2017 Dec:217(6):633-641. doi: 10.1016/j.ajog.2017.07.025. Epub 2017 Jul 22 [PubMed PMID: 28743440]
Ghi T, Eggebø T, Lees C, Kalache K, Rozenberg P, Youssef A, Salomon LJ, Tutschek B. ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2018 Jul:52(1):128-139. doi: 10.1002/uog.19072. Epub [PubMed PMID: 29974596]
Benedetti TJ, Lowensohn RI, Truscott AM. Face presentation at term. Obstetrics and gynecology. 1980 Feb:55(2):199-202 [PubMed PMID: 7352081]
Ducarme G, Ceccaldi PF, Chesnoy V, Robinet G, Gabriel R. [Face presentation: retrospective study of 32 cases at term]. Gynecologie, obstetrique & fertilite. 2006 May:34(5):393-6 [PubMed PMID: 16630740]
Cruikshank DP, Cruikshank JE. Face and brow presentation: a review. Clinical obstetrics and gynecology. 1981 Jun:24(2):333-51 [PubMed PMID: 7307363]
Domingues AP, Belo A, Moura P, Vieira DN. Medico-legal litigation in Obstetrics: a characterization analysis of a decade in Portugal. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2015 May:37(5):241-6. doi: 10.1590/SO100-720320150005304. Epub [PubMed PMID: 26107576]
. Intrapartum care for healthy women and babies. 2022 Dec 14:(): [PubMed PMID: 32212591]
Use the mouse wheel to zoom in and out, click and drag to pan the image

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
The PMC website is updating on October 15, 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Pan Afr Med J
Management of face presentation, face and lip edema in a primary healthcare facility case report, Mbengwi, Cameroon
Nzozone henry fomukong.
1 Microhealth Global Medical Centre, Mbengwi, Cameroon
2 Department of Medicine and Surgery, Faculty of Health Sciences University of Buea, Buea, Cameroon
Ngouagna Edwin
Mandeng ma linwa edgar, ngwayu claude nkfusai.
3 Department of Microbiology and Parasitology, Faculty of Science, University of Buea, Buea, Cameroon
4 Cameroon Baptist Convention Health Services (CBCHS), Yaoundé, Cameroon
Yunga Patience Ijang
5 Department of Public Health, School of Health Sciences, Catholic University of Central Africa, Box 1110, Yaoundé, Cameroon
Joyce Shirinde
6 School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria Private Bag X323, Gezina, Pretoria, 0001, Pretoria, South Africa
Samuel Nambile Cumber
7 Institute of Medicine, Department of Public Health and Community Medicine (EPSO), University of Gothenburg, Box 414, SE - 405 30 Gothenburg, Sweden
8 Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
Face presentation is a rare obstetric event and most practitioners will go through their carriers without ever meeting one. Face presentation can be delivered vaginally only if the foetus is in the mentum anterior position. More than half of the cases of face presentation are delivered by caesarean section. Newborn infants with face presentation usually have severe facial oedema, facial bruising or ecchymosis. These syndromic facial features usually resolved within 24-48 hours.
Introduction
Face presentation is a rare unanticipated obstetric event characterized by a longitudinal lie and full extension of the foetal head on the neck with the occiput against the upper back [ 1 - 3 ]. Face presentation occurs in 0.1-0.2% of deliveries [ 3 - 5 ] but is more common in black women and in multiparous women [ 5 ]. Studies have shown that 60 per cent of face presentations have one or more of the following risk factors: small fetus, large fetus, high parity, previous caesarean section (CS), contracted pelvis, fetopelvic disproportion, cord around the neck multiple pregnancy, hypertensive disorders of pregnancy, polyhydramnios, uterine or nuchal cord anomaly. But 40 per cent of face presentations occur with none of these factors [ 6 , 7 ]. A vaginal birth at term is possible only if the fetus is in the mentum anterior position. More than half of cases of face presentation are delivered by caesarean section [ 4 ]. Newborn infants with face presentation usually have severe facial edema, facial bruising or ecchymosis [ 8 ]. Repeated vaginal examination to assess the presenting part and the progress of labor may lead to bruises in the face as well as damage to the eyes.
Patient and observation
Case presentation: a 21 year old primigravida at 40 weeks gestation from the last normal menstrual period referred to our facility for prolonged second stage of labor after visiting two health centres. She labored for a total of 14hrs, membrane ruptured spontaneously 12hrs before referral. Amniotic fluid was documented by midwife to be clear. She attended antenatal clinics in Mbengwi health centre 5 times, was diagnosed of hepatitis B during antenatal consultations, received no treatment. She did not do any ultrasound due to financial constraints. On examination, she was healthy, in painful distress, blood pressure 131/76mmhg, pulse 85 beats/min, temperature 37.2 o C SPO2 98%. On abdominal exams, uterus was gravid, fundal height 35cm, lie longitudinal, fetal heart rate 137bpm, cephalic presentation, engaged 2/5, with moderate contractions of 2 in 10 minutes. On vaginal examination, cervix was fully dilated, membranes ruptured, presenting part was face, mentum anterior. The conclusion made was mento-anterior face presentation ( Figure 1 ). Paturient was counseled, labor was augmented with 1 amp of oxytocin in 500ml of glucose 5% and started at 10drops/mins. Ten minutes later she delivered a male baby with Apgar score 6/10, 8/10 on the first and fifth minute. The baby weighed 3.2kg, length was 50cm, and head circumference was 41cm. Syndromic facial appearance with marked edema at the baby's lips, face and scalp was evident and he had bruising on the right nasolabial groove and right cheeks ( Figure 2 ). Physical examination of the infant's respiratory system, cardiovascular system, and his abdominal examination were normal, as was his neurological examination. Placenta was delivered by controlled cord traction 5mins later with all cotyledons. Delivery was complicated by a second degree perineal tear. Perineal tear was repaired with absorbable suture under local anaesthesia. Estimated blood lost was 350ml. baby received Hepatitis B immunoglobulins, hepatitis B vaccine and vitamin K were administered to the baby. 24 hours later, facial swellings resolved ( Figure 3 ), baby breast feeds well. Baby and mother were discharged on day 3 postpartum all fine.

Men-tum anterior face presentation

Bruising, marked lip and facial edema

Baby 24 hours later with all syndromic facial features resolved
Ethics : informed consent: written informed consent was obtained from the patient's parents for the publication of this case report.
Face presentation is a rare obstetric event and most practitioner will go through their carriers without ever meeting one [ 3 ]. We presented a case of face presentation noticed in the delivery room on digital examination in a patient with no risk factors. In a poor resource setting as ours where ultrasound is not readily available, this event is often scary and confusing to most midwives and nurses. This may prompt repeated vaginal exams for confirmation of presentation. This intend will lead to bruising of the baby's face and delay effective management [ 8 ]. Exact knowledge about the fetal position and level is important for providing the correct management of this malpresentation. When face presentation is diagnosed, around 60% of cases are in the mentum anterior position, 25% are mentum posterior and 15% are mentum transverse [ 5 ]. The patient presented the most common form of face presentation (mentum anterior). Labor was augmented, vaginal delivery was attempted and successfully conducted. Facial bruising, lip and face edema are very common complication of face presentation. These complications usually resolve within 24-48 hours [ 9 , 10 ] in this case facial edema completely resolved within 24hours ( Figure 3 ) and baby breastfeed well.
Repeated vaginal exams should be avoided when presenting part is unsure. Vaginal delivery should be attemped only on mentum anterior face presentation, in other cases, emergency ceserian section should be performed. Syndromic facial features in babies born from face presentation resolve completely within 24-48 hours.
Competing interests
The authors declare no competing interests.
Acknowledgements
We thank the participant of this study.
Authors’ contributions
NHF, NE, MMLE, NCN, YPI, FB, JS and SNC conceived the case series, assisted with the study design and participant enrollment, designed the study protocol and collected the data. NE, MMLE, NCN and SNC assisted in interpretation of results and wrote the manuscript. All authors read and approved the final manuscript.
- Face Presentation

Face it. We have a lot to learn about fetal positioning. The old paradigm is fetal positions are random. The new paradigm is that babies match the space available.
Face and brow presentations occur when baby’s spine extended until the head is shifted back so baby’s face comes through the pelvis first.
Baby may settle in a face or brow presentation before labor or they may become a face or brow presentation, usually when a posterior baby has it’s chin pushed further up by the pelvic floor during descent.
A baby who is in a face-first or forehead-first position often started as an extended (chin up) occiput posterior or occiput transverse position. Coming down on to the pelvic floor with the forehead leading then “converted” this baby’s head to the face first position.
The baby’s face may be bruised for a couple days after the birth. The brow presentation may cause a redness but only occasionally will cause a bruise.
Mobility of the pelvis and the freedom of maternal movements often help bring the face-first baby down through the pelvis with good strong, uterine surges.
But not always. Sometimes the labor can’t move baby down. Cesareans are more common, but a portion of the higher surgical rate is because time is not given to the mother to begin or continue labor, or to be out of bed for this labor. Monitoring becomes important. Expect a bit of an unusual heart rate to contraction pattern seen in these labors.
- When is Breech an Issue?
- Belly Mapping® Breech
- Flip a Breech
- When Baby Flips Head Down
- Breech & Bicornuate Uterus
- Breech for Providers
- What if My Breech Baby Doesn't Turn?
- Belly Mapping ®️ Method
- After Baby Turns
- Head Down is Not Enough
- Sideways/Transverse
- Asynclitism
- Oblique Lie
- Left Occiput Transverse
- Right Occiput Anterior
- Right Occiput Posterior
- Right Occiput Transverse
- Left Occiput Anterior
- OP Truths & Myths
- Anterior Placenta
- Body Balancing
What makes labor easier for a face-first baby and you?
Balance the body and the baby will thank you by curling into position to aim, not their face, but the crown of their head.
Flexion is physiological. So support physiology and the baby will change their position. We may need a little physics.
In Labor with a Face or Brow Presentation
Back baby up!
Forward-leaning Inversion with a jiggle of the buttocks right through 1-2 contractions often backs baby up so they can tuck their chin. Then they can aim into the pelvis with an easier position.

A little effort can make labor a lot easier!
Only after baby’s crown is first, then do Side-lying Release in labor.
Before Labor with a face or brow presentation
Face presentation may reflect a psoas/pelvic floor imbalance with a collapse in the front body.
Free the piriformis, strengthen the buttocks, lengthen the hamstrings, squat for lengthening the pelvic floor, don’t worry about strengthening the pelvic floor right now. Alignment, walking, stabilizing and lengthening will tone the pelvic floor. Use it by breathing with your whole body.
Before labor, it’s safe to do Side-lying Release when baby’s face-first head isn’t in the pelvis yet.
Free the way
The psoas is the upper guide, the pelvic floor is the lower guide. release spasms and lengthen both.
Make room for the baby by releasing muscles that spasm, lengthen ligaments that are shortened, and support the abdominal muscles by attending to the muscles that interact with them, don’t go directly to the front first.
Featured Products
Shop spinning babies®.
For additional education to even further enhance your pregnancy and labor preparation, shop our extensive collection of digital downloads, videos, DVDs, workbooks, and more.

Connect with Us
Sign up for our newsletter:, more information:.
Have any questions or concerns? Email us at [email protected]

Get the New
Spinning babies® small physio ball.
- Non-toxic PVC
- Heavy metals free
- Phthalate free

- 2022 New Pearls of Exxcellence Articles
Management of Brow, Face, and Compound Malpresentations
Author: Meera Kesavan, MD
Mentor: Lisa Keder MD Editor: Daniel JS Martingano DO MBA PhD
Registered users can also download a PDF or listen to a podcast of this Pearl. Log in now , or create a free account to access bonus Pearls features.
Fetal malpresentation, including brow, face, or compound presentations, complicates around 3-4% of all term births. Because these abnormal fetal presentations still are cephalic, many such cases result in vaginal deliveries, yet there are increased risks for adverse outcomes, including cesarean delivery resultant surgical complications, persistent malpresentation precluding vaginal delivery, and abnormal labor resulting in arrest of dilation or descent.
These fetal malpresentation are differentiated in the following ways:
- In face presentations, the presenting part is the mentum, which is further divided based on its position, including mentum posterior, mentum transverse or mentum anterior positions. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Mentum anterior malpresentations can potentially achieve vaginal deliveries, whereas mentum posterior malpresentations cannot.
- In brow presentations, there is less extension of the fetal neck as in face presentations making the leading fetal part being the area between the anterior fontanelle and the orbital ridges. These presentations are uncommon and are managed similarly to face presentations. Brow presentation can be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
- Compound presentation is defined as the leading fetal part, including a fetal extremity, alongside a cephalic or breech presentation. Management of compound presentations is expected (and often incidentally noted following delivery) because the extremity will often either retract as the head descends or will feasibly allow for delivery in its current position, with manipulation attempts to reduce the compound presentation usually avoided.
Risk factors for brow and face presentations include fetal CNS malformations, congenital or chromosomal anomalies, advanced maternal age, low birthweight, abnormal maternal pelvic anatomy (e.g. contracted pelvis, cephalopelvic disporotion, platypelloid pelvis, etc.) and nulliparity. non-Hispanic White women have the highest risk for malpresentation, whereas non-Hispanic Black women have the lowest risk.
Diagnosis usually is made during the second stage of labor while performing routine vaingla examinations and involves palpation of the abnormal leading fetal part (forehead, orbital ridge, orbits, nose, etc.) Obstetric ultrasound can additionally provide complimentary information to support these diagnoses and distinguish from other fetal malpresentations or malpositions. In face presentation, the mentum (chin) and mouth are palpable.
Management considerations for face, brow, and compounds presentations are unique with compound presentations having higher rates of vaginal delivery and lower complications as compared to either brow or face presentations.
- For brow presentations, approximately 30-40% of brow presentations will convert to a face presentation, and about 20% will convert to a vertex presentation. Anterior positions have the possibility of vaginal deliveries and can be managed by usual labor management principles, whereas mentum posterior positions are indications for cesarean delivery.
- For face presentations, the likelihood of vaginal delivery depends on the orientation of the mentum, with mentum anterior being most suitable for vaginal delivery. If the fetus is mentum posterior, flexion of the neck is precluded and results in the inability of fetal descent.
- For compound presentations, management is expectant and manipulation of the leading extremities should be avoided. Most cases of compound presentation result in vaginal deliveries. For term deliveries, compound presentations with parts other than the hand are unlikely to result in safe vaginal delivery.
Labor management for brow and face presentation overall involves continuous fetal heart rate monitoring and repeat clinical assessments, given the increased potential of fetal complications as noted. Caution should be used with internal monitoring devices, which can cause ophthalmic injury or trauma to the presenting fetal parts, with the use of fetal scalp electrodes discouraged and intrauterine pressure catheters acceptable with appropriate clinical judgment and feasibility.
Midforceps, breech extraction, and manual manipulation are not recommended and increase the risk of maternal and neonatal morbidity.
Neonatal outcomes for both face and brow presentations include facial edema, bruising, and soft tissue trauma. Complications of compound presentation specifically include umbilical cord prolapse and injury to the presenting limb. With appropriate management, neonatal and maternal morbidity for face, brow, and compound presentations are low.
Further Reading:
Bar-El L, Eliner Y, Grunebaum A, Lenchner E, et al. Race and ethnicity are among the predisposing factors for fetal malpresentation at term. Am J Obstet Gynecol MFM. 2021 Sep;3(5):100405. doi: 10.1016/j.ajogmf.2021.100405. Epub 2021 Jun 4. PMID: 34091061.
Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017 Dec;217(6):633-641. doi: 10.1016/j.ajog.2017.07.025. Epub 2017 Jul 22. PMID: 28743440 .
Pilliod RA, Caughey AB. Fetal Malpresentation and Malposition: Diagnosis and Management. Obstet Gynecol Clin North Am. 2017 Dec;44(4):631-643. doi: 10.1016/j.ogc.2017.08.003. PMID: 29078945 .
Zayed F, Amarin Z, Obeidat B, et al. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet. 2008 Nov;278(5):427-30. doi: 10.1007/s00404-008-0600-0. Epub 2008 Feb 19. PMID: 18283473 .
Initial Approval: August 2013; Revised: 11/2016; Revised July 2018; Reaffirmed January 2020; Revised September 2021. Revised July 2023.
This site uses cookies.

This feature is only available for registered users.
Log in here:, not a registered user.
Becoming a registered user gives you access to special features like PDF downloads and podcast episodes of each SASGOG Pearl of Exxcellence.
Create a Free Account
Are you sure you want to remove this Pearl from your favorites list?
Face presentation at term: incidence, risk factors and influence on maternal and neonatal outcomes
- Maternal-Fetal Medicine
- Published: 09 April 2024
- Volume 310 , pages 923–931, ( 2024 )
Cite this article

- Yongqing Zhang 1 na1 ,
- Tiantian Fu 1 na1 ,
- Luping Chen 1 ,
- Yinluan Ouyang 1 ,
- Xiujun Han 1 &
- Danqing Chen ORCID: orcid.org/0000-0002-0201-7215 1
160 Accesses
Explore all metrics
The incidence, diagnosis, management and outcome of face presentation at term were analysed.
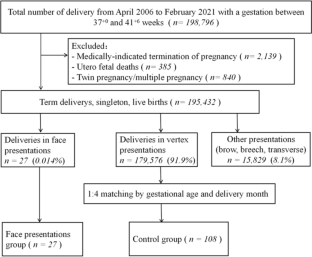
A retrospective, gestational age-matched case–control study including 27 singletons with face presentation at term was conducted between April 2006 and February 2021. For each case, four women who had the same gestational age and delivered in the same month with vertex position and singletons were selected as the controls (control group, n = 108). Conditional logistic regression was used to assess the risk factors of face presentation. The maternal and neonatal outcomes of the face presentation group were followed up.
The incidence of face presentation at term was 0.14‰. After conditional logistic regression, the two factors associated with face presentation were high parity (adjusted odds ratio [aOR] 2.76, 95% CI 1.19–6.39)] and amniotic fluid index > 18 cm (aOR 2.60, 95% CI 1.08–6.27). Among the 27 cases, the diagnosis was made before the onset of labor, during the latent phase of labor, during the active phase of labor, and during the cesarean section in 3.7% (1/27), 40.7% (11/27), 11.1% (3/27) and 44.4% (12/27) of cases, respectively. In one case of cervical dilation with a diameter of 5 cm, we innovatively used a vaginal speculum for rapid diagnosis of face presentation. The rate of cesarean section and postpartum haemorrhage ≥ 500 ml in the face presentation group was higher than that of the control group (88.9% vs. 13.9%, P < 0.001, and 14.8% vs. 2.8%, P = 0.024), but the Apgar scores were similar in both sets of newborns. Among the 27 cases of face presentation, there were three cases of adverse maternal and neonatal outcomes, including one case of neonatal right brachial plexus injury and two cases of severe laceration of the lower segment of the uterus with postpartum haemorrhage ≥ 1000 ml.
Conclusions
Face presentation was rare. Early diagnosis is difficult, and thus easily neglected. High parity and amniotic fluid index > 18 cm are risk factors for face presentation. An early diagnosis and proper management of face presentation could lead to good maternal and neonatal outcomes.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

Prognosis for deliveries in face presentation: a case–control study

Critical analysis of risk factors for intrapartum fetal death

“To get the baby out off the hook”: a prospective, longitudinal, multicenter, observational study about decision making in vacuum-assisted operative vaginal delivery
Explore related subjects.
- Medical Ethics
- Medical Imaging
Data availability
The original data can be provided by E-mail if needed.
Code availability
Cunningham FG, Williams JW (2018) Williams obstetrics, 25th edn. McGraw-Hill Medical, New York, pp 450–452
Google Scholar
Arsène E, Langlois C, Clouqueur E, Deruelle P, Subtil D (2019) Prognosis for deliveries in face presentation: a case-control study. Arch Gynecol Obstet 300:869–874. https://doi.org/10.1007/s00404-019-05241-6
Article PubMed Google Scholar
Cruikshank DP, Cruikshank RN (1981) Face and brow presentation. A review. Clin Obstet Gynecol 24:333–351. https://doi.org/10.1097/00003081-198106000-00003
Article CAS PubMed Google Scholar
Schwartz Z, Dgani R, Lancet M, Kessler I (1986) Face presentation. Aust N Z J Obstet Gynaecol 26:172–176. https://doi.org/10.1111/j.1479-828x.1986.tb01560.x
Bashiri A, Burstein E, Bar-David J, Levy A, Mazor M (2008) Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med 21:357–360. https://doi.org/10.1080/14767050802037647
Arsene E, Langlois C, Garabedian C, Clouqueur E, Deruelle P, Subtil D (2016) Prenatal factors related to face presentation: a case–control study. Arch Gynecol Obstet 294:279–284. https://doi.org/10.1007/s00404-015-3992-7
Tapisiz OL, Aytan H, Altinbas SK, Arman F, Tuncay G, Besli M et al (2014) Face presentation at term: a forgotten issue. J Obstet Gynaecol Res 40:1573–1577. https://doi.org/10.1111/jog.12369
Lau WL, Cho LY, Leung WC (2011) Intrapartum translabial ultrasound demonstration of face presentation during first stage of labor. J Obstet Gynaecol Res 37:1868–1871. https://doi.org/10.1111/j.1447-0756.2011.01650.x
Shaffer BL, Cheng YW, Vargas JE, Laros RK Jr, Caughey AB (2006) Face presentation: predictors and delivery route. Am J Obstet Gynecol 194:e10-12
Benedetti TJ, Lowenshon RI, Truscott AM (1980) Face presentation at term. Obstet Gynecol 55:199–202
CAS PubMed Google Scholar
Pilliod RA, Caughey AB (2017) Fetal malpresentation and malposition: diagnosis and management. Obstet Gynecol Clin N Am 44:631–643. https://doi.org/10.1016/j.ogc.2017.08.003
Article Google Scholar
Bellussi F, Ghi T, Youssef A, Salsi G, Giorgetta F, Parma D et al (2017) The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol 217:633–641. https://doi.org/10.1016/j.ajog.2017.07.025
Ducarme G, Ceccaldi PF, Chesnoy V, Robinet G, Gabriel R (2006) Face presentation: retrospective study of 32 cases at term. Gynecol Obstet Fertil 34:393–396. https://doi.org/10.1016/j.gyobfe.2005.07.042
De Bernardo G, Svelto M, Giordano M, Sordino D (2017) Face presentation in delivery room: what is strategy? BMJ Case Rep. https://doi.org/10.1136/bcr-2016-219114
Article PubMed PubMed Central Google Scholar
Manning JB, Tolcher MC, Chandraharan E, Rose CH (2015) Delivery of an impacted fetal head during cesarean: a literature review and proposed management algorithm. Obstet Gynecol Surv 70:719–724. https://doi.org/10.1097/OGX.0000000000000248
Download references
Acknowledgements
The authors wish to acknowledge Menglin Zhou, Zhengyun Chen and Guohui Yan for their valuable assistance for the manuscript.
No specific funding was obtained for this study.
Author information
Yongqing Zhang and Tiantian Fu have contributed equally to this work.
Authors and Affiliations
Department of Obstetrics, School of Medicine, Women’s Hospital, Zhejiang University, 1st Xueshi Road, Hangzhou, 310006, Zhejiang, People’s Republic of China
Yongqing Zhang, Tiantian Fu, Luping Chen, Yinluan Ouyang, Xiujun Han & Danqing Chen
You can also search for this author in PubMed Google Scholar
Contributions
YZ: conceptualization, methodology, writing—original draft. TF: conceptualization, formal analysis, writing—original draft. LC: data collection, follow-up. YO: investigation, resources. XH: investigation, formal analysis, supervision. DC: conceptualization, writing—review and editing, supervision. All authors read and approved the final manuscript.
Corresponding authors
Correspondence to Xiujun Han or Danqing Chen .
Ethics declarations
Conflict of interest.
All authors have no conflicts of interest to disclose.
Ethics approval
Our study was planned in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Local Ethics Committee of the Women’s hospital, school of medicine, Zhejiang university ( Ethical No. IRB-20210211-R ).
Consent for publication
Consent to participate.
As this was a retrospective study, written informed consents were not obtained, but all patients’ records/information were anonymized before analysis. The images used in this paper (Figs. 1 , 2 , 3 ) were given informed consent by the pregnant woman.
Human and animal rights
This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Zhang, Y., Fu, T., Chen, L. et al. Face presentation at term: incidence, risk factors and influence on maternal and neonatal outcomes. Arch Gynecol Obstet 310 , 923–931 (2024). https://doi.org/10.1007/s00404-024-07406-4
Download citation
Received : 09 July 2023
Accepted : 28 January 2024
Published : 09 April 2024
Issue Date : August 2024
DOI : https://doi.org/10.1007/s00404-024-07406-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Face presentation
- Risk factors
- Brachial plexus injury
- Postpartum haemorrhage
- Find a journal
- Publish with us
- Track your research
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Diagnosis and management of face presentation
- PMID: 7005774
Face presentation is an unusual complication of pregnancy; it occurs once in every 500 to 600 deliveries. Prematurity, fetal macrosomia, anencephaly, and cephalopelvic disproportion (CPD) are the major obstetric factors that predispose the fetus to face presentation. Although the mechanisms of labor in face presentation are different from those of simple vertex presentation, there is no consistent alteration in the duration of labor in the absence of underlying CPD. When disproportion does not exist and gross anomalies are not present, the prognosis for spontaneous vaginal delivery is excellent. The majority of perinatal losses reported in face presentation have resulted from traumatic operative vaginal deliveries, specifically version and extraction and midforceps rotations. Recent experience at this institution with a limited series of face presentations demonstrates that, with careful intrapartum surveillance, delivery can be accomplished with no increase in risk to either mother or fetus.
PubMed Disclaimer
Similar articles
- A simple measure to enhance atraumatic vaginal delivery of vertex-presenting fetuses in prematurity. Sherer DM. Sherer DM. Am J Perinatol. 1992 May;9(3):162-3. doi: 10.1055/s-2007-999312. Am J Perinatol. 1992. PMID: 1575835
- Face and brow presentation in northern Jordan, over a decade of experience. Zayed F, Amarin Z, Obeidat B, Obeidat N, Alchalabi H, Lataifeh I. Zayed F, et al. Arch Gynecol Obstet. 2008 Nov;278(5):427-30. doi: 10.1007/s00404-008-0600-0. Epub 2008 Feb 19. Arch Gynecol Obstet. 2008. PMID: 18283473
- [Normal delivery in deflected presentations. Presentation of the face, presentation of the forehead]. Jahier J. Jahier J. Rev Prat. 1975 Jan 11;25(3):163-6, 169-70, 175-6. Rev Prat. 1975. PMID: 1118709 French. No abstract available.
- Labor with abnormal presentation and position. Stitely ML, Gherman RB. Stitely ML, et al. Obstet Gynecol Clin North Am. 2005 Jun;32(2):165-79. doi: 10.1016/j.ogc.2004.12.005. Obstet Gynecol Clin North Am. 2005. PMID: 15899353 Review.
- Controversies: selective vaginal delivery for breech presentation. Erkkola R. Erkkola R. J Perinat Med. 1996;24(6):553-61. J Perinat Med. 1996. PMID: 9120738 Review.
- Management of face presentation, face and lip edema in a primary healthcare facility case report, Mbengwi, Cameroon. Fomukong NH, Edwin N, Edgar MML, Nkfusai NC, Ijang YP, Bede F, Shirinde J, Cumber SN. Fomukong NH, et al. Pan Afr Med J. 2019 Aug 8;33:292. doi: 10.11604/pamj.2019.33.292.18927. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692903 Free PMC article.
Publication types
- Search in MeSH
Related information
Linkout - more resources, full text sources.
- Ovid Technologies, Inc.
- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Joker 2 Could Feature The Birth Of A New Franchise

Your changes have been saved
Email is sent
Email has already been sent
Please verify your email address.
You’ve reached your account maximum for followed topics.
Joker 2's Box Office Might Be A Repeat of Another DC Disaster
Joker 2 review by someone who has seen it early makes a bold claim, an mcu star confirms that reshoots were needed to save captain america 4, key takeaways.
- The possibility of a Joker 3 remains uncertain, as Todd Phillips focused on releasing Joker: Folie à Deux.
- Fans hoped to see Two-Face in the Joker 2 but were disappointed; however, a more grounded version remains a possibility.
- If Phillips decides to explore Two-Face further, it could provide a realistic and compelling take on the character without the need for extreme physical transformations.
Now that audiences are finally getting another look at Todd Phillips' version of the Joker in his new film, it's officially time to start wondering what might come next. It's an open question as to whether Joker: Folie à Deux is the end of a franchise or the middle movie in what could eventually become a trilogy. Phillips hasn't talked about whether Joker 3 might be a possibility just yet, as he's been focusing on getting the Joaquin Phoenix and Lady Gaga-starring film out the door.
If Joker 2 is the end of this franchise, it doesn't have to be Phillips' final movie using DC Comics as the basis for these more reality-based versions of classic villains . It's possible that Phillips already has the model for his next project. It's even possible he wanted to tease audiences with the character and leave them wanting quite a bit more, by not offering what many people hoped would be the big reveal in Folie à Deux.

According to early estimates, things are not looking good for Joker 2, and might earn much less than its predecessor in the opening weekend.
Joker 2 Might Not Be The End Of This Story

When the trailers for Joker 2 first launched, fans of the new franchise were quite excited to see one lawyer talking to the media amid what appeared to be a trial for Arthur Fleck, aka The Joker. It took no time at all for audiences to put two and two together and correctly guess the attorney was none other than Assistant District Attorney Harvey Dent . Dent of course is better known to DC Comics fans as Two-Face. Some people even wondered whether Phillips would introduce the new character as part of the action for Folie à Deux . However, long before the film hit theaters, the director made it clear there wasn't any intention of introducing another iconic criminal to the movie; having Dent be the man who was prosecuting Fleck was simply too good an opportunity to pass up. He said as much in an interview with IGN earlier this fall. In the same breath, Phillips shot down the hopes of millions that Dent would become Two-Face in this film.
"But it’s not about his – we don’t really reveal his dark side. We see a young Harvey Dent."
While Phillips didn't offer up the villain that so many hoped would make an appearance, there's no guarantee that Harvey Dent won't eventually turn into that character in a future film. The biggest question would be how it would happen. One of the things that has people wanting the director to take on this character is how he routinely offers the "real world" version of the larger than life crimals .
Arther Fleck doesn't fall into a vat of chemicals, he doesn't get his face chopped up, and he doesn't turn into the "clown price of crime" overnight. We get to see how one of the most beloved bad guys can really be born. He's just someone who at first, is rather tragic . He even seems like a genuinely nice, if strange person before he decides that it's more fun to be bad. The same is done with Harley Quinn, who is usually portrayed as even more of a cartoonish figure than the joke himself. But in Phillips' version of the character, she's really just a woman who has some issues of her own and gravitates to Fleck for reasons that some people could absolutely see happening in the real world.
A More Grounded Two-Face Could Be Compelling

If Todd Phillips does decide to launch a Two-Face movie from Harvey Dent's appearance in Joker 2, it seems like it could work quite well in the same way that Matt Reeves ' The Penguin series on Max is working. It could offer up a real world look at a character that is over the top in some ways but is far more ground than even Arthur Fleck's Joker in others. At his core, Two-Face is a very understandable and relatable person.
At his core, Two-Face is a very understandable and relatable person.
Harvey Dent is someone who has put some much pressure on himself that in the end, he cracks. He wants so much to be a good person that his personality splinters. In most of the movies, it happens with some sort of horrific accident as the catalyst, but there are plenty of people out in the real world who go bad simply because of something internal.
Phillips has not said whether he will work on another movie like this.
The Todd Phillips version of Two-Face wouldn't need to have half his face burned away like Aaron Eckhart's version of the character did in The Dark Knight . It could simply be a man who flips his personality the same way he flips a coin to make decisions. In fact, that would make the character quite a bit more interesting as the ugliness inside of him isn't quite so obvious. Add in the fact that someone who makes his bones by trying some of the most famous criminals in a major city, turning to a life of crime will always be interesting, and Phillips, should he decide to go to another franchise along the lines of Joker: Folie à Deux it could end up being even more popular and really start a chain reaction that could allow for deep dives into other DC heroes and villains with a more realistic feel.

An early Joker 2 review makes a bold claim about Joaquin Phoenix and Lady Gaga's upcoming movie that will likely excite DC fans even more.

COMMENTS
Face and brow presentation is a malpresentation during labor when the presenting part is either the face or, in the case of brow presentation, it is the area between the orbital ridge and the anterior fontanelle. This activity reviews the evaluation and management of these two presentations and explains the interprofessional team's role in ...
Face Presentation Causes & Risk Factors. These conditions may increase the likelihood of a face presentation birth: A Very Big Baby (Fetal Macrosomia): Larger babies may have trouble fitting into the birth canal in the standard position, leading to alternative presentations. Prematurity: Premature infants are more likely to have non-standard presentations, including face presentation, because ...
Presentation refers to the part of the fetus's body that leads the way out through the birth canal (called the presenting part). Usually, the head leads the way, but sometimes the buttocks (breech presentation), shoulder, or face leads the way. Position refers to whether the fetus is facing backward (occiput anterior) or forward (occiput ...
When a baby is head down, face down, the medical term for it is the cephalic occiput anterior position. This the most common position for a baby to be born in. With the face down and turned slightly to the side, the smallest part of the baby's head leads the way through the birth canal. It is the easiest way for a baby to be born.
Face Presentation: Definition: Face presentation occurs when the baby's face is positioned to lead the way through the birth canal instead of the vertex (head). Causes: Face presentation can occur due to factors such as abnormal fetal positioning, multiple pregnancies, uterine abnormalities, or maternal pelvic anatomy.
In a face presentation, the fetal head and neck are hyperextended, causing the occiput to come in contact with the upper back of the fetus while lying in a longitudinal axis. The presenting portion of the fetus is the fetal face between the orbital ridges and the chin. The fetal chin (mentum) is the point designated for reference during an ...
The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face (figure 1A-B), or brow (figure 2) [1]. Diagnosis and management of face and brow presentations will be reviewed here. Other cephalic malpresentations are ...
Fetal presentation, or how your baby is situated in your womb at birth, is determined by the body part that's positioned to come out first, and it can affect the way you deliver. At the time of delivery, 97 percent of babies are head-down (cephalic presentation). But there are several other possibilities, including feet or bottom first (breech ...
The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference. Face presentation is an abnormal form of cephalic presentation where the presenting part is the mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back.
Face presentation is an abnormal form of cephalic presentation where the presenting part is the mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. In brow presentation, the neck is not ...
A vaginal birth at term is possible only if the fetus is in the mentum anterior position. More than half of cases of face presentation are delivered by caesarean section . Newborn infants with face presentation usually have severe facial edema, facial bruising or ecchymosis . Repeated vaginal examination to assess the presenting part and the ...
Occiput or cephalic anterior: This is the best fetal position for childbirth. It means the fetus is head down, facing the birth parent's spine (facing backward). Its chin is tucked towards its chest. The fetus will also be slightly off-center, with the back of its head facing the right or left. This is called left occiput anterior or right ...
The baby's face may be bruised for a couple days after the birth. The brow presentation may cause a redness but only occasionally will cause a bruise. Mobility of the pelvis and the freedom of maternal movements often help bring the face-first baby down through the pelvis with good strong, uterine surges. But not always.
Vertex Presentation. A vertex presentation is the ideal position for a fetus to be in for a vaginal delivery. It means the fetus is head down, headfirst and facing your spine with its chin tucked to its chest. Vertex presentation describes a fetus being head-first or head down in the birth canal.
Cephalic occiput posterior. Your baby is head down with their face turned toward your belly. This can make delivery a bit harder because the head is wider this way and more likely to get stuck ...
In face presentation, the mentum (chin) and mouth are palpable. Management considerations for face, brow, and compounds presentations are unique with compound presentations having higher rates of vaginal delivery and lower complications as compared to either brow or face presentations. For brow presentations, approximately 30-40% of brow ...
A total of 61 women who met the study criteria were diagnosed with face presentation in labor; for 55 of the women, follow-up data were available for analysis. Cases of face presentation were abstracted from a cohort of 40,598 cases, which gave an incidence rate of 1 in 666. Preterm delivery, birth weight <2500 g, and maternal obesity were more ...
Face presentation is a rare event characterized by a longitudinal lie and full extension of the fetal head on the neck with the occiput against the upper back [].Its incidence varies from 0.5 to 3 per 1000 births, according to previous series [1,2,3,4,5,6].Causes of face presentation are numerous, generally stemming from any factor that favours extension or prevents head flexion.
Brow presentation is a rare complication, which affects only one in every 500 to one in every 1,400 births. So the chances of it happening are low. If a brow presentation is picked up in early labour, your baby may still flex her head in time for the birth. Alternatively, she may tip her head further back and be born face first.
Birth complications: Some examples of birth complications include needing an emergency C-section or your obstetrician needing to use forceps or a vacuum to deliver your baby. Bleeding too much (postpartum hemorrhage) or having a large vaginal tear could also cause physical birth trauma.
Abstract. Face presentation is an unusual complication of pregnancy; it occurs once in every 500 to 600 deliveries. Prematurity, fetal macrosomia, anencephaly, and cephalopelvic disproportion (CPD) are the major obstetric factors that predispose the fetus to face presentation. Although the mechanisms of labor in face presentation are different ...
Please verify your email address. The possibility of a Joker 3 remains uncertain, as Todd Phillips focused on releasing Joker: Folie à Deux. Fans hoped to see Two-Face in the Joker 2 but were ...